Army rolls out simpler, lighter software to operational medical forces

Domains
March 6, 2020
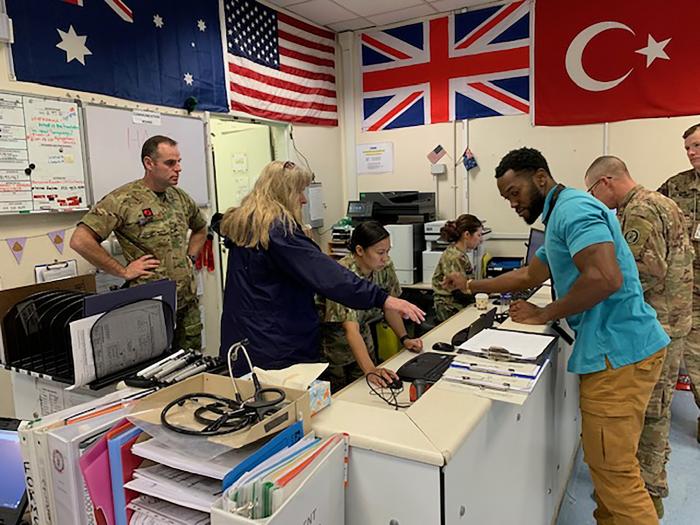
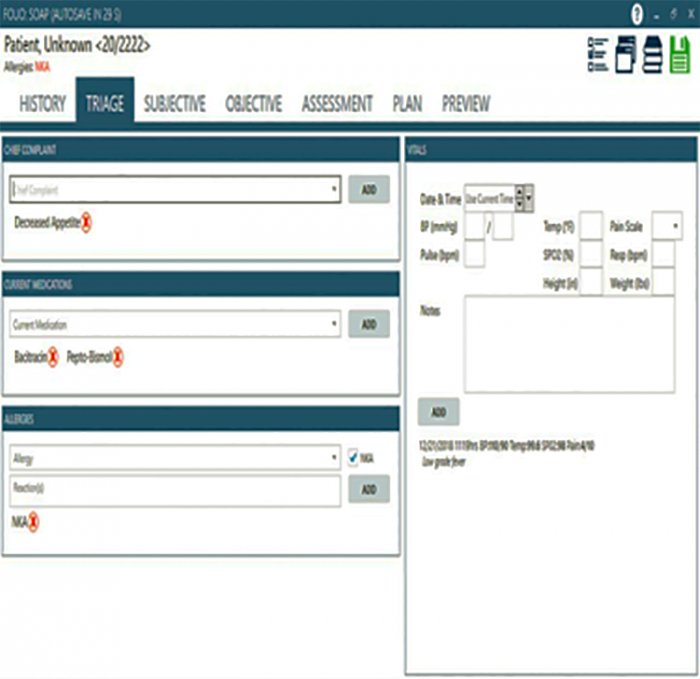
FORT DETRICK, Md. -- In November 2019, the Army deployed its Health Assessment Lite Operations (HALO) software to medical forces in Afghanistan. HALO is a digitized version of the Standard Form (SF) 600 used by DoD medical personnel to document patient treatment for wounded, injured or sick patients. It was developed by the Medical Communications for Combat Casualty Care (MC4), the Army acquisition program with primary responsibility for providing Army operational health IT capabilities for deployed medical forces. The current version of HALO is designed primarily for documenting out-patient treatment at Role 1 battalion aid stations and at Role 2 military treatment facilities (MTFs).
Due to the success of the HALO deployment, Army leaders will begin rolling out HALO to medical forces worldwide during the remainder of 2020 and the first quarter of 2021.
HALO was initially piloted to Army medical units in Romania and Bulgaria in September 2018. On November 15, 2019, it went live and deployed to the Role 2 MTF in Kabul, Afghanistan. This was an important deployment, as it not only enabled MC4 engineers to evaluate HALO’s effectiveness at a Role 2 MTF near the battlefront, but it also allowed the MC4 team time to assess additional features needed for future HALO enhancements. U.S. and Allied medical providers, after receiving less than two hours of training, were able to document patient encounters using HALO. In the first two days of use, three times as many electronic patient encounters were documented than in the two weeks leading up to the HALO “go live” date using the legacy software, Armed Forces Health Longitudinal Technology Application – Theater (AHLTA-T).
According to Mr. Tracy Ellis, product director for MC4, the launch of HALO exceeded expectations and “validated HALO as an application that can be deployed quickly to fulfill the critical mission of electronically capturing patient health data in operational settings.” This real-world deployment provided the MC4 team the opportunity to receive feedback from providers regarding ease of use and adequacy of training, and to identify requirements to incorporate into the next version of HALO.
Through the end of January, more than 1,000 patient encounters have been documented electronically using HALO by both U.S. and NATO providers, according to MC4. Many of these encounters would have been documented previously on paper.
In a post-deployment survey, MC4 asked clinicians about their level of satisfaction with HALO. Feedback received from medical staff indicates a high degree of interest with HALO over AHLTA-T. “The beauty of HALO is its simplicity. It is easy to use and overall it’s a vast improvement over AHLTA-T,” described Maj. Paul Schunk, an emergency care physician.
When asked if she would rather go back to using the legacy AHLTA-T after using the HALO application, Capt. Lesley Tarongoy, an emergency room nurse, gave an emphatic “NO.” The same answer was given by all survey respondents when asked the same question.
Sgt. Kenneth Roberts, an Army medic with 2nd battalion, 3rd Security Force Assistance Brigade, described HALO as “self-correcting… and a system that’s easily broken down,” in describing the features and user interface. When asked what he thought overall, Roberts remarked, “very satisfied.”
To learn more about these developments, and to follow up on the next steps for HALO as an Army OHIT solution, I sat down with Tracy Ellis and the MC4 engineers in charge of its development.
Clark: First, before we get into HALO as a software solution, can you tell me about electronic health records and why they are important to operational medical forces?
Ellis: It’s all about taking care of Soldiers, Sailors, Airmen, Marines, and other deployed personnel. Documenting health care for deployed service members is a critical part in continuity of care, patient safety, and ensuring that proper medical care is provided when they leave the service. Electronic documentation has many advantages over paper records. When there is network connectivity, EHRs can be transmitted in seconds and are then viewable by medical personnel with network access. Electronic records aren’t easily lost when compared to paper records. Information in the electronic record can be data mined to support medical research and to provide leadership with near real-time information for use in decision making. We want to achieve the same high quality health record – whether deployed or at home station. Finally, a comprehensive, lifelong electronic health record provides medical information to ensure that the service member gets the right care at the right time – both while they are in the service and when their care transitions to the VA or civilian sector upon their separation from service.
Clark: What operational challenges does this present?
Ellis: Electronic documentation in a deployed environment presents a number of challenges. The number one issue is that network communications are not always available or can become degraded – the term used by the military is “disconnected, intermittent, or low bandwidth” (DIL). That is why there’s a requirement that deployed operational health IT systems have the ability to continue to document health care in a DIL environment. While the legacy AHLTA-T software provides this capability, it depends on a server to store the patient encounter. If the connection between the provider’s computer (a.k.a. client) and the server is lost, it requires reconfiguring the provider’s computer as a client-server to operate in this environment. This is normally handled by deployed personnel with systems administration expertise– who may or may not even be co-located with you. HALO was designed specifically to allow electronic documentation to continue and then forward the patient encounters once communications are restored, with no additional steps required.
Clark: If HALO is designed for situations with low bandwidth, or when network communications go out, can you explain more about how that works; perhaps provide a scenario?
Ellis: Much like your internet and cable in your home, the time it takes to install your cable connection, like for issues such as weather, technical issues, user error, and low bandwidth, can all affect your service. Take all of these factors, then add in potential for disruption of the communications network by our adversary, and you can see examples that could create a DIL environment that could last from a few minutes to a few days or longer.
Clark: You recently began HALO deployment in Afghanistan. How did that go?
Ellis: Our HALO deployment in Afghanistan was actually the second time HALO’s been used in the field. In September 2018, we deployed HALO to several Army units deployed in Eastern Europe. After several months of use by units in Bulgaria and Romania, we took lessons learned from that deployment and used the agile fielding approach to software development to make changes to HALO prior to deploying an updated version to Afghanistan in November 2019.
The November deployment to Afghanistan exceeded our expectations. Forty-one hospital staff members (20 U.S., 21 NATO) received two hours of HALO training prior to ”go live.” Most were able to document patient care electronically using HALO without further assistance from the HALO training team. Prior to deploying HALO, NATO providers and many U.S. providers rarely used the legacy AHLTA-T software, as it was too hard to learn during their 90-120 day deployments.
Clark: Do you see HALO used with other application advancements, say telehealth?
Ellis: Yes. If virtual health is involved, that information is still documented in HALO and becomes part of the patient’s record. So it is compatible with telemedicine advances.
Clark: Can providers communicate with each other through the application? Can you explain a bit about its capabilities?
Ellis: HALO allows a patient encounter to be open and accessible to other providers who may have a requirement to also provide documentation or co-sign. An example might be the physician who is documenting notes while a medic is continuing to monitor and document vital signs. HALO provides an alert any time more than one individual is documenting in the open patient encounter. The current health care software does not allow more than one individual to access the open encounter.
Clark: So how does HALO save the Army money?
Ellis: Because HALO is simple and easy to use, the savings are realized by reducing the number of hours spent on training. Since HALO is so easy to support, it will allow IT personnel to spend more of their time supporting other applications. The small size of the HALO application compared to the legacy application has the potential to reduce hardware costs.
Clark: As an Army acquisition program, what are you doing to support the Army’s leadership priorities and support multi-domain operations? In other words, how does MC4 remain relevant?
Ellis: The deployment and further development of HALO supports the Army’s priorities – readiness, modernization and reform. Advances in operational health information systems, such as HALO, provide real-time data in support of medical mission command. This helps maintain Readiness through the ability to rapidly shift resources in support of the fight. HALO is fit-for-purpose, lightweight, and agile enough to rapidly modify as required. While the focus of this interview is on HALO and electronic health care documentation, the MC4 program deploys operational health IT solutions that support all 10 health care functions, including logistics, preventive medicine, and medical mission command. In each of these areas, lightweight, scalable, cost effective solutions that incorporate commercial-off-the-shelf hardware and software solutions are being developed to deliver capability in support of multi-domain operations ranging from early entry operations through large-scale combat operations. And the rapid, incremental delivery of capability are consistent with Modernization and Reform efforts by leveraging power of operational health information systems to help maintain the Army’s competitive edge.
Clark: Isn’t the DoD already moving out with modernizing its EHRs? Why not just use that solution in the deployed environment rather than develop an application like HALO?
Ellis: MHS Genesis is military medicine’s modernized, enterprise-level electronic health record that has also been adopted by the VA. But it is not ready to field to operational forces. Until it is ready, being satisfied with the legacy operational health care applications is not the answer, especially when there are opportunities to get enhancements and additional capabilities in the interim to our deployed Soldiers. We see HALO as a cost effective improvement over the legacy EHR that can serve as a bridging solution until MHS Genesis is ready to deploy to operational forces. That is still projected to be 3-5 years from now.
(Brent Hunter, Cybersecurity Chief, MC4)
Clark: Are there cybersecurity risks with deploying an application like HALO?
Hunter: There are no protected health information/personally identifiable information (PHI/PII) security issues with any of the products MC4 supports. As part of the risk management framework (RMF) process, MC4 uses the PHI/PII overlay that specifically addresses security controls as they relate to PHI/PII data. The protection of PHI/PII is done in layers to provide a robust security posture for the HALO system. Access to the PHI/PII is controlled through roles and permissions that only authorized personnel can set up and manage. Data in transit and at rest is encrypted and in compliance with all Army/DoD cybersecurity requirements.
Clark: How do you overcome the lengthy RMF/ATO/ATC processes?
Hunter: There is really no way of overcoming the time it takes to complete the RMF/ATO/ATC process. Once we receive an Authority to Operate (ATO) via the RMF process, we begin working on the Authority to Connect (ATC). This process can't begin until we receive the ATO. However, once we complete the process, both the ATO and ATC are valid for three years. We leverage the change management process to introduce new capabilities, as long as those capabilities don't introduce vulnerabilities or impact the security of the MC4 system.
(Jay Patnaude, Technical Management Division Chief, MC4)
Clark: What is the data transfer rate, e.g. how many encounters can be pushed at the same time? Where does the data go?
Patnaude: Our system is designed for DIL environments for the medic. The transfer of the medical encounters is seamless. Regardless if the medic has connectivity or not, HALO is designed to constantly monitor for a connection and when it has one, it automatically bursts medical encounters to the HALO hub it’s connected with. The HALO hub will then transmit encounters to theater medical data store and the clinical data repository, the Soldier's lifelong electronic health record. HALO has the ability to send data in any format to any medical system that it’s allowed to communicate with.
Clark: Is HALO software and hardware compatible with AHLTA-T and other applications?
Patnaude: HALO is lightweight and easy to maintain at only 90MB in size. It’s designed to work with AHLTA-T and can communicate with any other application. It’s also what we call hardware agnostic.
Clark: Is the training intensive? Do you anticipate an app for making training accessible to medics or providers?
Patnaude: No. HALO was specifically designed to be easy to use. A good way to think about it is that we used the simplicity of how apps work on your smart phone to design the HALO interface. There are training materials for HALO, however, most medics pick up how to use HALO in five to ten minutes.
Clark: It’s really that easy?
Patnaude: Yes. In fact, from what we’ve seen so far, after that initial interaction, we just let the medics explore the HALO application and answer questions as they come up. We’ve been seeing they intuitively get it after only a few minutes of use.
Clark: Does HALO require a lot of support?
Patnaude: No. HALO is designed to be updated remotely by pushing software to the locations throughout theater. If a unit is not on the network, then we can send them one disc and the unit can easily patch or upgrade the system.
Clark: Finally, what if you lose a device in the field that’s loaded with the HALO app, is there some kind of remote wipe?
Patnaude: HALO is installed on self-encrypting drives that will allow the system to purge itself after so many failed attempts to access it. If the laptop can be located on the network, then yes we can also wipe it remotely. It's also important to note that HALO data is transmitted to TMDS and the CDR, so patient information should not remain on a HALO system for long periods of time. After data has been sent, there are purging processes that remove older records from the HALO system on a regular interval.
Clark: Defender 2020 and HALO’s Future
Patnaude: Due to the success of the November 2019 launch, worldwide deployment of HALO to Army units will continue through the remainder of 2020. HALO will be used for Role 1 and Role 2 out-patient electronic documentation during the Defender 2020 exercise in Europe. Defender 2020 will be the largest exercise conducted in Europe in more than 25 years. Tens of thousands of U.S. troops will take part in this division-sized exercise to help the Army practice drawing equipment, coordinating communications and mission command, and moving personnel across six countries in the European theater. This will be a true test of HALO, with hundreds of medical personnel spread across the area of operations documenting patient care during the exercise.
Related News
-
Onedia James: a logistician and leader with a family legacy of service
April 22, 2025Onedia James recently stepped into the role of acting deputy project manager for Army Data and Analytics Platforms (ARDAP) at U.S. Army Program Executive Office (PEO) Enterprise, where she helps oversee and support the data portfolio’s four programs. -
PEO Enterprise’s new PL Digital Market reimagines IT product/service procurement
April 2, 2025FORT BELVOIR, Va. – U.S. Army Program Executive Office (PEO) Enterprise today announced the launch of the Product Lead (PL) Digital Market, which replaces PL Computer Hardware, Enterprise Software and Services (CHESS), effective Apr. 2, 2025. -
Two vastly different Army programs prepare for Software Acquisition Pathway
March 24, 2025At U.S. Army Program Executive Office Enterprise, which is now over two years into its Agile transformation, several enterprise software programs are already in the execution phase of the DOD’s Software Acquisition Pathway, which is designed to facilitate rapid and iterative delivery of software capability to users.
Work for Us
Join a winning team! Search for job opportunities with PEO Enterprise.
Work with Us
Help support important missions. Explore ways your company can work with PEO Enterprise.